
When Rest Isn’t Enough: Could Your ‘Chronic Burnout’ Actually Be Undiagnosed ADHD?
You've rested, reduced your hours, done everything right — and still hit a wall. This article explores why chronic burnout in high-performing women and expats is sometimes misread as a lifestyle problem, when the missing piece may actually be undiagnosed ADHD. ADHD coach Yann Ghisalberti breaks down the hidden cost of masking, what ADHD really looks like in adult women, and why the biological and neurological pieces of burnout recovery need to work together.
By Yann Ghisalberti, ADHD Coach
You’ve done the blood tests. You’ve prioritized sleep. You’ve even taken a sabbatical or reduced your hours at work. And yet, the "wall" is still there. You wake up exhausted, and the simplest tasks, like responding to an email or deciding what’s for dinner, feel like climbing a mountain.
We often explore how biological "missing pieces" like iron deficiency or thyroid issues can keep you stuck in fatigue. But there is another invisible factor that frequently masquerades as chronic burnout, especially in high-performing women and expats: Undiagnosed ADHD.
If you feel like you are "failing" at recovery, it might not be because you aren't resting enough. It might be because your brain is running a marathon every single day just to appear "normal" and to process every thought and manage all daily issues.
The "Cost of Repression": Why Rest Doesn't Fix Masking
Many women with ADHD reach adulthood without an ADHD diagnosis because they have become experts at resilience and at masking.
I often discuss the "Cost of Repression", the internal energy tax you pay to try harder and harder, to hide your struggles, mimic neurotypical behavior and over-compensate for perceived "laziness".
When you have ADHD, your brain’s executive functions (the management system for planning, focusing, and regulating emotions) work differently. To keep up with the demands of a career and motherhood, you likely rely on high-octane fuel: stress, adrenaline, overexertion and perfectionism. Eventually, the tank runs dry. This isn't just "work stress", it’s a neurological burnout. If you don't address the underlying ADHD, resting is like trying to refill a bucket with a hole in the bottom.
ADHD as It Truly Is vs. As It Is Seen
We often think of ADHD as the 'hyperactive little boy', a myth I explore in my 'Problem Child' article.
But for many women, ADHD looks like:
Internal Restlessness: A mind that never shuts off even when the body is paralyzed with fatigue.
Decision Fatigue: Spending two hours "recovering" on the sofa because the mental load of choosing a task was too high.
The Shame Cycle: Feeling like you should be able to handle a "normal" life leading to the belief that you are just "not trying hard enough."
As I explore in my article ADHD as it is often seen vs. as it truly is, ADHD isn't a deficit of attention; it’s a challenge in regulating it. When you are burnt out, this regulation breaks down completely.
The Hormonal Missing Link
There is a powerful synergy between the work Nerys does and ADHD coaching. We know that dopamine (the primary neurotransmitter involved in ADHD) is heavily influenced by estrogen.
Many women find that their ADHD symptoms and their burnout become unbearable during perimenopause or specific points in their hormonal cycle. When estrogen and progesterone fluctuate, it impacts dopamine levels and the "ADHD brain" loses its ability to cope. This is why a biological approach (like Nerys’s focus on hormones and nutrition) and a neurological approach (ADHD strategies) must go hand-in-hand. Understanding your hormonal journey is vital to understanding why your brain feels like it’s "on fire."
Diagnosis as a "Way Forward"
Many people fear a label, but as an expat coach, I see a diagnosis as a protective key. It moves you from "What is wrong with me?" to "How does my brain work?"
If you are a high-performer who has hit a wall that rest won't fix, consider looking beyond the physical fatigue. You might not be "broken" or "lazy." You might just have a brain that requires a different manual.
Are you ready to stop fighting your brain and start working with it?
If this resonates, I invite you to explore the Post-Burnout Reset™ or book a discovery call on my website to see if neurodivergence is the missing piece in your recovery puzzle.
About the author
Yann Ghisalberti is a certified ADHD Coach and the founder of Coach4ADHD, based in Amsterdam. After a 15-year career in the fast-paced world of IT, Yann pivoted to coaching following his own ADHD diagnosis in the Netherlands. He specializes in helping high-performing expats and neurodivergent families navigate the unique challenges of living abroad while working with their brains instead of against them. Yann is the creator of The Post-Burnout Reset™, a 12-week neuroscience-based program designed to help professionals recover from burnout and regain career clarity through an ADHD-friendly lens.
Find him at coach4adhd.nl/
Connect with Yann here: Book a Free Discovery Call

Iron Deficiency and Fatigue: Why Your Blood Test May Be Missing the Full Picture
Persistent fatigue, brain fog, hair loss? Low iron — even without anaemia — could be a root cause your standard blood test isn't catching. Here's what to ask for.
Persistent fatigue, brain fog, hair loss? Low iron — even without anaemia — could be a root cause your standard blood test isn't catching. Here's what to ask for.
If you wake up tired even after a full night's sleep, feel like daily life has become heavier than it used to be, and notice things like hair falling out in the shower, a short walk leaving you more breathless than it should, or a persistent foggy feeling that follows you through the day — iron deficiency may be worth exploring. Because unlike many contributors to long-term fatigue, this one is both identifiable and treatable. I know this firsthand. For years I pushed through exhaustion while managing work, family, and the everyday demands of life — assuming it was just my lot. When an iron deficiency was eventually identified, supplementing changed things in ways I hadn't expected. My energy came back. The low-level anxiety lifted. And perhaps most meaningfully: I had something left in the evenings to actually be present with my children.
In this article:
Gut health and iron levels are linked
What iron deficiency actually is — and the type most often missed
What low iron does to your body, thyroid, and mood
What you can do, and what to ask your GP
Your gut and your iron levels are more connected than you might think
Poor gut health — whether through low-grade inflammation, changes to the microbiome, or a compromised intestinal lining — can significantly reduce how much iron your body actually absorbs, even if you are eating iron-rich foods regularly. When the gut lining is disrupted, inflammatory signalling molecules enter the bloodstream and affect other organs, contributing to a persistent fatigue that doesn't lift with rest. The gut is not just a bystander in iron deficiency. For some women, it is the reason the deficiency exists in the first place. This is an important connection that rarely comes up in standard consultations — and it is one reason why addressing gut health and nutrient status together often unlocks progress that neither approach achieves alone.
What iron deficiency actually is — and the type most often missed
Iron is central to the production of haemoglobin, the protein in red blood cells that carries oxygen to every tissue and organ in the body. It is also stored inside cells as part of a protein called ferritin, which acts as the body's iron reserve. This gives us two distinct clinical pictures: Iron deficiency anaemia (IDA): both haemoglobin and ferritin are low Non-anaemic iron deficiency (NAID): haemoglobin is normal, but ferritin — stored iron — is low Iron deficiency anaemia currently affects approximately 1.2 billion people worldwide. Non-anaemic iron deficiency is estimated to be at least twice as common — and it is the type most likely to be missed. A recent review published in the Canadian Medical Association Journal puts it plainly: "Iron deficiency without resulting anemia, or NAID, is associated with fatigue, reduced work performance, and reduced cognitive function. Iron deficiency is the most common cause of anemia despite being preventable and easily treated." [1] A routine blood count may come back entirely normal, and yet someone can be running on depleted iron reserves — with real, measurable consequences for how they feel and function every day.
Why your results might be "normal" and still be a problem
Even when anaemia is absent, low ferritin can produce symptoms indistinguishable from full iron deficiency anaemia: fatigue, brain fog, poor exercise tolerance, low mood, and hair loss. Yet ferritin is routinely left out of standard blood panels. Current clinical guidance is shifting on this. The same CMAJ review specifies: "Treatment is indicated when ferritin is below 50 µg/L in a pregnant person, below 30 µg/L in other adults, and below 20 µg/L in children." [1] Many integrative practitioners go further, suggesting a target of at least 50 µg/L for all adults — though this is something to explore with your GP in the context of your individual results. The practical implication is straightforward: if you have only ever had your haemoglobin checked, you may not have the full picture.
What low iron does to your body — beyond tiredness
Iron's role in the body extends well beyond red blood cells, which is why its deficiency can show up in such varied and seemingly unrelated ways.
Thyroid function
Iron is essential for the activity of thyroid peroxidase, an enzyme that catalyses the production of thyroid hormones. Iron deficiency has been associated with impaired thyroid hormone production and increased prevalence of thyroid autoimmunity, particularly in women of reproductive age [2]. This matters because hypothyroid symptoms and iron deficiency symptoms overlap considerably — fatigue, cold sensitivity, weight changes, brain fog — and without testing both, the picture can remain frustratingly unclear.
Mood and mental health
Iron is a cofactor for the enzymes responsible for producing serotonin, dopamine, and noradrenaline — the neurotransmitters most closely linked to mood regulation. Research suggests its role in neurotransmission is not sufficiently considered by practitioners [3], and that iron status should be routinely assessed in people presenting with depression or persistent low mood, particularly in women and in cases that have not responded well to standard treatment.
What you can do: a practical starting point
Step 1: Get the right tests
Ask your GP to test both haemoglobin and ferritin. It is also worth requesting CRP (C-reactive protein), a marker of inflammation. Ferritin is an acute-phase protein that can appear falsely elevated when inflammation is present, so CRP provides an important control for interpreting your results accurately.
Step 2: Understand your results in context
If your ferritin or haemoglobin is low, prescribed supplementation is usually necessary to bring levels up to a meaningful threshold. Dietary changes alone are unlikely to be sufficient if levels are significantly depleted — particularly in menstruating women, where ongoing iron loss makes it difficult to rebuild stores from food alone.
Step 3: Support absorption through diet
Regular intake of iron-rich foods remains a valuable foundation, for example:
Red meat and organ meats
Beans and lentils (black beans, chickpeas)
Dark leafy greens (spinach, kale)
Pumpkin seeds
Pairing these foods with a source of vitamin C — a squeeze of lemon, orange juice, some peppers, or tomatoes — increases iron absorption meaningfully. Some evidence suggests that properties of tea and coffee can reduce absorbption, so if you’re struggling to get your levels up then you may want to avoid these near the time you eat or when you take your supplements. It is also worth noting that haem iron from animal sources is considerably more bioavailable than non-haem iron from plant sources.
Iron is one piece of a larger picture
Persistent fatigue rarely has a single cause. Iron deficiency is one of the most common and most overlooked contributors — but it sits alongside thyroid function, hormonal changes, vitamin D, B12, gut health, and other factors that are worth exploring systematically. For many of the women I work with, mapping out these possible biological contributors is the first time anyone has taken a thorough look at the full picture. And what often follows is a significant shift — not just in energy, but in how they understand what has been happening in their bodies. The fatigue wasn't in their head. It wasn't a failure to manage stress well enough. There was something biological that hadn't been found yet. If that resonates with your experience, a discovery call is a good place to start. 👉 Book a free discovery call at savourcoaching.com/appointments
References
1. Leung, A. et al. (2025). Diagnosis and management of iron deficiency in females. Canadian Medical Association Journal. PMC12237530. This review outlines the clinical significance of both anaemic and non-anaemic iron deficiency, and provides updated ferritin thresholds for diagnosis and treatment.
2. Li, M. et al. (2021). Iron Deficiency, a Risk Factor of Thyroid Disorders in Reproductive-Age and Pregnant Women: A Systematic Review and Meta-Analysis. Frontiers in Endocrinology. PMC7947868. This meta-analysis demonstrates that iron deficiency significantly increases the risk of thyroid autoimmunity and impaired thyroid hormone production in women of reproductive age
3. Berthou, C. et al. (2022). Iron, neuro-bioavailability and depression. eJHaem. PMC9175715. This paper explains the mechanistic link between iron deficiency and depression through impaired neurotransmitter synthesis, and calls for iron status to be assessed as part of standard depression workups.
Could Your Gut Health Be Contributing to Fatigue or Burnout?
Fatigue and burnout are often viewed as purely mental or lifestyle issues. We may assume we’re simply working too hard, not sleeping enough, or juggling too many responsibilities.
But what many people don’t realise is that gut health can play an important role in how we experience energy, stress, and recovery from burnout.
During my recent gut health workshops in Utrecht, this topic resonated strongly with participants. Many people shared that they experience both digestive symptoms and ongoing fatigue, yet rarely hear about how closely these systems are connected.
Research increasingly shows that gut health, the gut microbiome, stress hormones and blood sugar regulation all influence our energy levels and resilience to burnout.
Understanding these connections can be a powerful first step toward improving both gut health and overall wellbeing.
Gut Health, the Microbiome and Energy
Inside our digestive system lives a vast community of microorganisms known as the gut microbiome. These trillions of bacteria help digest food, produce vitamins, regulate inflammation, and support the immune system. SavourCoaching_GutHealthPresent…
But the gut does much more than process food.
It communicates constantly with the brain through the gut–brain axis, a network involving nerves, hormones, and immune signals. Because of this connection, changes in stress levels can influence digestion — and changes in gut health can affect mood, energy levels, and mental clarity.
This is one reason people experiencing fatigue or burnout often report symptoms such as bloating, food sensitivities, brain fog, and low energy alongside digestive discomfort.
Why Fatigue and Digestive Symptoms Often Appear Together
Digestive symptoms such as bloating, reflux, constipation, diarrhoea, or food sensitivities are very common. In the Netherlands, around one in four people experience gut-related issues.
At the same time, many people experiencing burnout report physical symptoms such as:
persistent fatigue
brain fog
unstable energy levels
digestive discomfort
food intolerances
This overlap is not a coincidence.
Chronic stress can alter digestion, influence the balance of the gut microbiome, and disrupt hormone regulation. Over time, these changes can affect nutrient absorption, inflammation levels, and energy production.
At the same time, an imbalanced gut microbiome can contribute to fatigue, mood changes, and reduced resilience to stress.
The Triangle of Hormonal Health
One framework I often use when discussing these connections with clients is the Triangle of Hormonal Health (source: www.functional-wellness.co.uk).
This model describes the interaction between three important regulatory systems in the body:
Stress and the nervous system
Blood sugar regulation
Sex hormones
These systems constantly influence one another. When one side of the triangle becomes unstable, the others can be affected as well.
It’s important to say that this triangle is just one lens through which we can view health. We could just as easily look at things from the perspective of gut health as a central system supporting many others, including the immune system, hormones, and the nervous system.
However, I find the triangle a particularly helpful framework when thinking about my clients’ symptoms in a holistic way. Fatigue, digestive issues, mood changes, and hormonal fluctuations often make more sense when we consider how stress, blood sugar regulation, and hormones interact.
Interestingly, many of the dietary changes that help stabilise blood sugar — such as balanced meals, fibre-rich foods, and regular eating patterns — are also extremely supportive for the gut microbiome. In other words, a way of eating that supports metabolic balance often ends up supporting gut health too.
The Hormonal Hierarchy: Why Cortisol and Insulin Matter
Closely related to the triangle is another useful concept: the Hormonal Hierarchy.
This hierarchy describes how certain hormones act as foundational regulators, influencing many other hormonal systems in the body.
At the base of the hierarchy sit two key hormones:
Cortisol and insulin.
Cortisol is the body’s main stress hormone. It helps us respond to challenges by mobilising energy and increasing alertness. However, when stress becomes chronic and cortisol remains elevated for long periods, it can disrupt digestion, sleep, immune function, and energy levels.
Insulin regulates blood sugar and determines how the body uses or stores energy from food. Large swings in blood sugar can lead to energy crashes, cravings, inflammation, and fatigue.
When cortisol and insulin are repeatedly out of balance, the body prioritises short-term survival rather than long-term repair. This can influence hormones further up the hierarchy, including thyroid hormones, reproductive hormones, and sleep-related hormones such as melatonin.
Because digestion is closely connected to both stress and blood sugar regulation, the gut is often one of the first systems to show signs of imbalance.
Supporting Gut Health for Better Energy
Improving gut health rarely comes from a single quick fix. Instead, it often involves small, sustainable changes that support both the microbiome and the body as a whole.
Some important foundations include:
eating a wide variety of plant foods to nourish beneficial gut bacteria
including fermented foods such as yoghurt, kefir, or sauerkraut
supporting stable blood sugar through balanced meals
managing stress and supporting the nervous system
prioritising sleep and recovery
Every person’s gut microbiome is unique, which means there is rarely a one-size-fits-all solution.
Looking Beyond Symptoms: A Holistic Approach to Gut Health and Burnout
One of the key messages from my workshops is that digestive health cannot be separated from the rest of the body. The gut is closely connected to our nervous system, hormones, immune function, and energy metabolism.
When someone experiences persistent fatigue, burnout, or digestive symptoms, it can be helpful to explore the bigger picture — including stress, nutrition, sleep, and possible biological root causes.
Persistent fatigue, burnout, and digestive symptoms are often signals that the body’s systems are under strain. By looking at gut health, stress regulation, and blood sugar balance together, it becomes possible to understand symptoms more clearly and support the body’s natural ability to restore energy and resilience.
Burnout or Perimenopause?
Fatigue, brain fog or burnout in your 40s? Learn how perimenopause can reduce resilience and amplify stress — and why recovery may feel harder now.
Perimenopause can look like fatigue.
It can also look like brain fog, poor sleep, irritability, anxiety, low mood, weight changes, loss of motivation, or a heavy, sluggish feeling in the body.
In other words, it can look exactly like what many women are told is burnout.
This symptom overlap is one of the main reasons perimenopause is often missed or mislabelled as burnout — by women themselves and sometimes by healthcare providers.
When burnout is part of the picture — but not the whole story
For many women, work really is demanding.
Long hours, responsibility, emotional labour, and sustained mental load can lead to genuine work-related burnout. Acknowledging this matters.
At the same time, many women notice that their ability to cope has changed.
Stress feels heavier. Recovery takes longer. Things that were once manageable suddenly aren’t.
This often leads to questions like:
Why does work affect me more than it used to?
Why does burnout feel deeper or harder to recover from this time?
Questions many women begin asking
As fatigue and emotional depletion persist, many women start to wonder:
Could I be burned out from work — but also physically less resilient than before?
Has something changed in my body that makes stress hit harder now?
Is there something underneath this fatigue that isn’t only related to my work environment?
These questions don’t deny burnout. They reflect a sense that the full picture hasn’t yet been explored.
Where perimenopause fits in
Perimenopause is a hormonal transition phase that can begin years before menopause, often while menstrual cycles are still regular.
For many women, symptoms start in the early to mid-40s, though they can appear earlier. Perimenopause commonly lasts 4–8 years.
During this phase, oestrogen and progesterone levels fluctuate rather than decline steadily. These fluctuations affect systems involved in:
energy regulation
sleep quality
mood and anxiety
cognitive function and brain fog
stress response and recovery
Research suggests that 70–80% of women experience symptoms during perimenopause, and many of these are psychological or cognitive — not just physical symptoms like hot flushes.
As hormonal patterns change, the body’s physiological resilience to stress can decrease. This means that even if work and life demands stay the same, coping and recovery may feel much harder.
For many women, this is the point where ongoing stress tips into a more serious or prolonged exhaustion — not due to weakness, but due to biological change.
Why burnout and perimenopause are often confused
Awareness of perimenopause is growing, but many women still reach this life stage without clear information about what it can feel like.
As a result, midlife fatigue is often explained as burnout alone — especially when work is demanding and routine blood tests fall within reference ranges.
What is frequently missed is how hormonal transition can amplify stress, reduce recovery capacity, and intensify burnout symptoms.
A more complete way of understanding midlife fatigue
For many women, the most accurate explanation isn’t burnout or perimenopause — it’s both.
Work stress may be the trigger.
Perimenopause may lower resilience.
Together, they can lead to fatigue, emotional depletion, and a sense of crisis.
Understanding this interaction often brings relief — because it finally makes sense.
What to explore with your GP
If fatigue, low mood, or burnout symptoms aren’t improving with rest or stress reduction alone, it may help to explore whether other factors are contributing.
Some women choose to ask about:
whether perimenopause could be relevant, even with regular cycles
whether iron status, thyroid function, or key nutrients have been reviewed
how stress and hormonal changes may be interacting
These conversations don’t require certainty — just clarity.
If this resonates
If you recognise yourself here, you’re not imagining things — and you’re not failing.
Burnout can be real. Perimenopause can be real. And sometimes, the combination is what turns pressure into exhaustion.
Understanding that context doesn’t solve everything — but it often changes what happens next.

Low Ferritin or Burnout? Why Iron Deficiency Is Often Missed
Low ferritin symptoms in women include fatigue, brain fog and low mood — even with normal haemoglobin. Learn why iron deficiency is often missed.
For many women, long-term fatigue is explained as burnout.
Work is demanding. Life is full. Recovery feels harder than it used to. Burnout often seems like the most reasonable conclusion.
But in a significant number of cases, exhaustion is not only — or not primarily — about stress.
It is linked to low ferritin, a sign of depleted iron stores that is frequently overlooked when haemoglobin levels are still normal.
When “normal” iron results don’t match how you feel
Iron status is commonly assessed using two markers:
Haemoglobin, which reflects whether there is enough iron to make red blood cells
Ferritin, which reflects iron stores — the body’s reserve
Many laboratories list ferritin values from around 20 µg/L (and sometimes lower) as “normal”.
When haemoglobin is normal and ferritin falls within this range, women are often reassured that iron deficiency is not the issue.
However, for many women, low ferritin symptoms appear well before anaemia develops.
Clinically, a large proportion of women do not feel well until ferritin levels reach around 50 µg/L or higher.
Iron deficiency without anaemia (IDWA)
Iron deficiency does not begin with anaemia.
There is often a prolonged phase where:
ferritin is depleted
haemoglobin remains within range
symptoms are already present
This is known as iron deficiency without anaemia (IDWA).
Because haemoglobin is normal, iron deficiency may be ruled out — even though iron-dependent systems throughout the body are already affected.
This is one of the main reasons low ferritin symptoms in women are missed.
Low ferritin symptoms in women that are frequently overlooked
Many healthcare providers are trained to recognise anaemia, but fewer are trained to recognise iron deficiency without anaemia.
As a result, symptoms are often attributed to stress, burnout, or mental health rather than low iron stores.
Common low ferritin symptoms in women include:
persistent fatigue or exhaustion
brain fog or poor concentration
low mood, anxiety, or apathy
reduced exercise tolerance
shortness of breath on exertion
dizziness or light-headedness
physical heaviness or weakness
hair shedding
frequent or lingering infections
These symptoms strongly overlap with those of anaemia — despite haemoglobin remaining normal.
Why low ferritin affects more than energy
Iron is often described as being important for oxygen transport, but its role in the body is much broader.
Iron is involved in:
cellular energy production
cognitive function and mental clarity
neurotransmitter activity related to mood and motivation
immune system function
This is why women with low ferritin often report brain fog, poor stress tolerance, low motivation, and frequent coughs or colds — even without anaemia.
When iron stores are depleted, the body may struggle to support multiple systems at once.
Why low ferritin is so often missed
Low ferritin is frequently missed because:
reference ranges are broad and symptom-blind
haemoglobin is prioritised over iron stores
symptoms are explained by lifestyle or stress
iron deficiency is only considered once anaemia appears
As a result, women may be told everything is “normal” — while continuing to feel unwell.
Over time, many adapt to functioning below their baseline, until exhaustion becomes severe enough to resemble burnout.
When burnout and low ferritin coexist
For many women, the question is not low ferritin or burnout — it is both.
Work stress increases energy demands.
Low ferritin reduces the body’s capacity to meet them.
Together, they can lead to:
reduced resilience
prolonged recovery
fatigue that does not resolve with rest alone
In this context, low ferritin does not replace burnout — it lowers the physiological buffer, making burnout more likely and harder to recover from.
What to explore with your GP
If fatigue or burnout symptoms persist, it may be helpful to explore iron status more closely — even if haemoglobin is normal.
Some women choose to ask:
what their ferritin level actually is (not just whether it’s “normal”
whether symptoms could reflect iron deficiency without anaemia
how ferritin results are being interpreted in relation to symptoms
whether ferritin levels around 20 µg/L are sufficient for optimal function
These conversations don’t require confrontation — just informed curiosity.
Why this understanding matters
When low ferritin is missed, women may spend years trying to improve their mental health when the problem is at least partly in the body — or, physiological.
Recognising low ferritin symptoms in women:
reduces self-blame
provides clarity
and often changes the direction of care
Burnout can be real.
Iron deficiency can be real.
And sometimes, addressing depleted iron stores is what finally allows recovery to begin.
Reference:
Cappellini MD, Musallam KM, Taher AT. Iron deficiency without anaemia: a diagnosis that matters. European Journal of Haematology. 2020.
Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC9692751/

Burnout, Iron Deficiency, and the Part of the Story I Was Missing
Long-term exhaustion isn’t always burnout. A personal story of missed iron deficiency, low ferritin, and what finally explained years of fatigue.
For a long time, I believed I was simply tired in the way adults are tired. The kind of tired that comes with work, children, responsibility, and getting older. I didn’t think something was wrong — I thought this was just life now.
But looking back, I can see how far from normal it really was.
I would wake up in the morning already exhausted, even after ten hours of sleep. I relied heavily on coffee just to get through the day, hoping each cup might finally do something. By late afternoon — still at work — the fatigue would hit hard. No amount of caffeine could touch it. My body felt heavy, my head foggy, I had hair loss and sometimes dizziness, and I was counting the minutes until I could go home.
I’d get through the evening routine with the kids, put them to bed, and then crash myself — far earlier than I wanted to. Evenings disappeared. There was no space for friends, no energy for hobbies, no exercise, no time for the basic life admin that quietly piles up when you’re always depleted. Everything became about getting through the day.
At some point, I started to accept this as my new normal.
I told myself it was my age. That it was life with kids and work. That maybe this was just how things would be from now on — permanently tired, permanently running on empty. What made it confusing was that I wasn’t neglecting myself. I wasn’t drinking excessively. I ate a healthy diet. I exercised when I could. I was doing all the things you’re supposed to do to “recover.”
And yet, nothing changed.
When people asked how I was, I said, “I’m fine.” Not because I was fine, but because explaining that level of exhaustion felt impossible. And because I didn’t want to hear the well-meaning responses: “Just take it easy,” or “It’ll get better when the kids are older.” I was already doing everything I could, and none of it was making a real difference.
There were moments that stayed with me. After returning to work, a colleague told me he wouldn’t bring me into his team because he assumed I’d just burn out again. Others seemed to think I was exaggerating how tired I was. That was hard to swallow — not just the fatigue itself, but the sense that it was becoming part of how I was seen.
Did I doubt myself? Yes and no. Part of me resigned myself to this being normal. But another part — quieter, persistent — kept wondering whether there was more to it. That’s why I kept reading, searching, and doing blood tests on my own. I didn’t have anyone guiding me through that process. I didn’t even know who could.
The real turning point came in an unexpected way: a Facebook group called The Iron Protocol. It sounds almost absurd now, but that group changed everything.
What I learned there was that the lower limits used for iron stores — ferritin — are often far too low to support good health. To feel well, ferritin typically needs to be around 50 µg/L or higher. Yet many lab ranges list anything above 20 µg/L as “normal.”
When I looked back at my own results, I was stunned. For five years, my ferritin had hovered between 20 and 30 µg/L — sometimes dropping even lower. No one had flagged it as a problem. In fact, it had likely worsened over time, partly due to endurance running and partly because I’d almost become vegetarian in an effort to improve my health.
Once I started appropriate treatment, the change was dramatic. Within about three months, my energy returned to what felt like normal. Not superhuman — just functional. Capable. Present.
And that’s when the anger hit.
I was angry that I’d been left unwell for so long. Angry about the years of unnecessary struggle. Angry about the time lost — time I could have spent feeling better, being more present with my children, living more fully. I hadn’t expected that grief, and I didn’t really know where to put it. It just felt deeply unfair.
Around that period, I had already left my job due to “burnout” and had retrained as a lifestyle coach and nutritionist. Food and health had always mattered deeply to me. But about six months ago, something clicked. I realised I could be the person I had needed — the one who helps women make sense of what’s happening when the burnout label doesn’t explain everything.
This wasn’t just my story. A close family member experienced something similar: severe iron deficiency, burnout leave, and eventually being pushed out of her job. I started seeing the same pattern again and again — women struggling, labelled, and left without real answers.
That’s what motivates me.
I don’t want women to stay stuck believing they’re broken, weak, or simply “not coping.” I don’t want exhaustion to quietly shrink lives while everyone assumes it’s inevitable. I believe there is often more going on — and that asking better questions sooner can change everything.
I used to believe my tiredness meant I was just getting older.
Now I believe it often signals an imbalance or dysregulation in the body.
If you’re reading this and you feel dismissed, I want you to know this: you’re not imagining it. There are people who can help. There is information out there. And you are allowed to keep asking questions — even the ones that feel obvious or “stupid.” No question is stupid when it comes to your health.
Keep advocating for yourself. You deserve answers.
The Hidden Biology Behind "Burnout": Why Mid-Career Women May Be Getting the Wrong Diagnosis
Rising burnout rates in women may mask iron deficiency, thyroid dysfunction and perimenopause. Why mid-career fatigue is often misdiagnosed.
Sarah*, a 41-year-old marketing executive, spent two years being treated for burnout. She'd tried therapy, meditation apps, and even a sabbatical. Nothing helped. It wasn't until a routine blood test revealed critically low iron stores that the pieces fell into place. Within months of proper treatment, her "burnout" vanished.
Sarah's experience highlights a concerning gap in how we diagnose fatigue in mid-career women. While workplace stress is real, there's growing evidence that biological conditions—particularly iron deficiency, thyroid dysfunction, and perimenopause—are being missed or diagnosed late, leaving women to struggle with treatable medical problems misattributed to psychological causes.
The Burnout Gender Gap: A Global Pattern
The scale of burnout among women is striking—and growing. In the Netherlands, burnout complaints surged from 11.3% in 2007 to 19.0% in 2023, with the increase particularly pronounced among women, those aged 25-35, and workers in healthcare and education. Swedish research reveals an even starker picture: 21.1% of women experience burnout compared to 12.8% of men, with women aged 40-49 showing the highest rates at approximately 25%.
Across North America, the pattern persists. In the United States, 46% of women report burnout compared to 37% of men—a gap that has more than doubled since 2019. A comprehensive analysis of 71 studies across 26 countries confirmed that women in healthcare professions endure significantly higher stress and burnout than their male colleagues. Even in China, female dental postgraduates show elevated rates of burnout, career choice regret, and depressive symptoms compared to male peers.
The burden is particularly heavy in Africa, where up to 80% of physicians in some countries report burnout, with women showing the highest scores. Among Moroccan oncology healthcare professionals, 61.5% experience severe burnout, with younger age and female gender identified as key risk factors.
Yet as burnout diagnoses soar, an uncomfortable question emerges: are we correctly identifying what's burning out—minds or bodies?
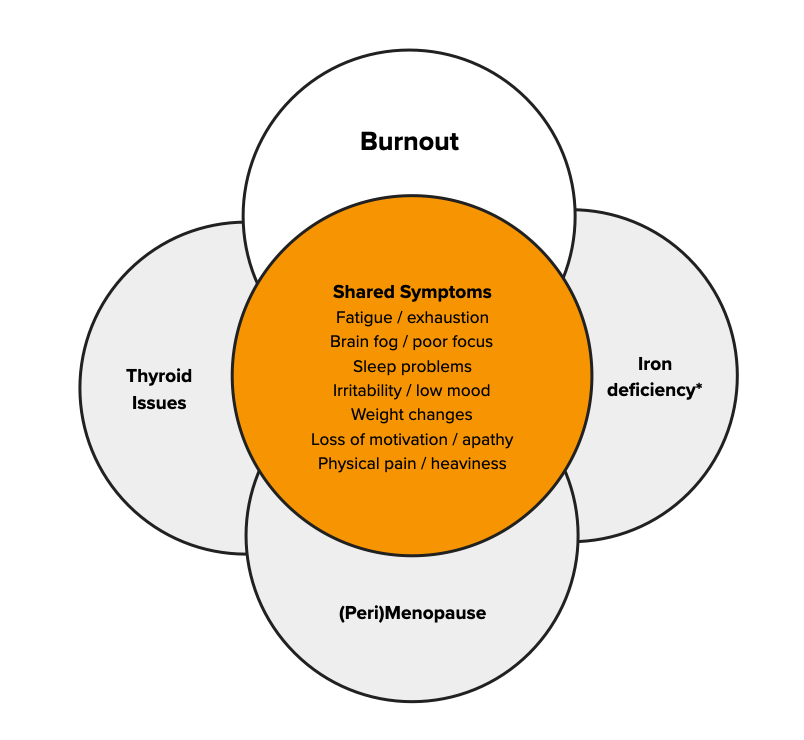
The Biological Triad
Iron Deficiency: The Misdiagnosed Epidemic
Iron deficiency affects 20-30% of menstruating women globally, yet its psychiatric impact remains dangerously underrecognized. In a Swiss study of 1,010 women diagnosed with iron deficiency, 35% initially received a different diagnosis—most commonly depression, burnout, anxiety, or chronic fatigue. These misdiagnoses led to unnecessary treatments and delayed appropriate care, leaving women symptomatic for months or years.
The mechanism is elegant but devastating. Iron is essential for oxygen transport, neurotransmitter synthesis, and cellular energy metabolism. When stores drop, cognitive function plummets—even before anemia develops. Studies demonstrate that iron-deficient women score significantly lower on attention, memory, and learning tasks, with improvements occurring within weeks of iron repletion.
Standard screening often fails these women. Many have "normal" hemoglobin but critically low ferritin (stored iron). Research shows ferritin below 30 μg/L impairs cognitive function, yet diagnostic thresholds are often set at 12-15 μg/L—catching only severe cases. Among young women and those with prior anemia, diagnostic delays are common as physicians order multiple iron treatment cycles before investigating underlying causes.
Thyroid Dysfunction: The Subtle Saboteur
Large observational studies reveal that 4-7% of community populations in the USA and Europe have undiagnosed hypothyroidism, with four in five cases being subclinical (elevated TSH with normal thyroid hormone levels). The symptoms—fatigue, weight changes, mood disturbance, cold intolerance, cognitive fog—overlap substantially with burnout.
The diagnostic challenge is compounded by age and sex. Research from Japan examining over 23,000 adults found that approximately 50% of women aged 30-39 diagnosed with subclinical hypothyroidism using standard reference ranges had normal thyroid function when age- and sex-specific ranges were applied. For women aged 60-69, this overdiagnosis rate reached 78%.
Meanwhile, true thyroid dysfunction goes unrecognized because symptoms are nonspecific. Fatigue is attributed to poor sleep or stress. Weight gain is blamed on lifestyle. Hair loss is dismissed as aging. The diagnosis often comes years late—if at all.
Perimenopause: The Diagnostic Black Hole
Perhaps no condition is more systematically misattributed than perimenopause. Women experiencing new-onset psychiatric symptoms during the menopausal transition face what researchers call "diagnostic overshadowing"—their symptoms are misdiagnosed as depression, anxiety, or in women with pre-existing mental illness, as relapse.
The statistics are sobering. Studies show seven of the eight conditions on the Patient Health Questionnaire depression scale (PHQ-8) can be caused by perimenopause or menopause, yet 25% of women aged 50-65 have never been told by their doctor that they're in this transition—even when 92% experienced menopausal symptoms in the past year.
Diagnosis is complicated by timing. Psychological symptoms typically precede physical ones by up to five years. A woman in her early 40s experiencing anxiety, irritability, insomnia, and cognitive changes may not yet have hot flashes or irregular periods—the "classic" signs clinicians expect. Research from multiple large cohort studies demonstrates that women with no history of depression are twice as likely to develop depressive symptoms during perimenopause, yet this knowledge hasn't translated into clinical practice.
The Interactive Triad: Why These Three Conditions Cluster
These conditions don't merely coexist—they interact. Iron deficiency impairs thyroid hormone metabolism and may worsen thyroid dysfunction. Perimenopause increases iron requirements while many women experience heavier menstrual bleeding, depleting iron stores. Thyroid dysfunction becomes more prevalent during the menopausal transition, with fluctuating estrogen affecting thyroid function.
A woman with all three conditions faces a multiplicative effect on symptoms. Her fatigue isn't just additive—it's synergistic. Her cognitive impairment compounds. Her emotional regulation crumbles. And when she seeks help, she's told she's burned out.
What Should Be Tested?
For women presenting with burnout symptoms, comprehensive evaluation should include:
Complete iron studies: Hemoglobin, ferritin, transferrin saturation, and iron. Ferritin below 30 μg/L warrants treatment even if hemoglobin is normal.
Comprehensive thyroid panel: TSH, free T4, free T3, and thyroid antibodies (TPO). Use age- and sex-specific reference ranges.
Reproductive hormone assessment in women 35+: FSH, estradiol, and consideration of cycle patterns to evaluate perimenopausal status.
The Path Forward
This isn't about dismissing psychological factors or workplace stress. Both are real, prevalent, and deserve attention. But when we default to psychological explanations for women's exhaustion without ruling out treatable biological conditions, we fail them twice—once by missing their diagnoses, and again by implying their suffering is somehow less "real."
Sarah's journey from misdiagnosed burnout to proper treatment isn't rare—it's disturbingly common. How many other "burned out" women are actually iron-deficient, hypothyroid, or perimenopausal? Until we routinely test for these conditions, we won't know. But the evidence suggests the number is substantial.
The question we should be asking isn't "Are you burned out?" It's "What's burning out—your mind or your biology?"
For Sarah, and countless women like her, the answer changed everything.
*Name changed to protect privacy
References
Alqahtani N, et al. (2019). Economic burden of symptomatic iron deficiency – a survey among Swiss women. BMC Women's Health, 19(1):38.
Cappellini MD, et al. (2020). Iron deficiency anaemia revisited. Journal of Internal Medicine, 287(2):153-170.
Hadine J, et al. (2024). Does menopause elevate the risk for developing depression and anxiety? Results from a systematic review. Menopause, 30(4).
Laurberg P, et al. (2021). Low awareness and under-diagnosis of hypothyroidism. Current Medical Research and Opinion, 37(12):2097-2106.
O'Brien KM, et al. (2023). Severe mental illness and the perimenopause. BJPsych Bulletin. PMC11669460.
Purvanova RK, Muros JP (2010). Gender differences in burnout: A meta-analysis. Journal of Vocational Behavior, 77(2):168-185.
Sholzberg M, et al. (2024). Diagnosis and management of iron deficiency in females. Canadian Medical Association Journal. PMC12237530.
Statistics Netherlands (2024). Trends in burnout complaints in the Netherlands 2007-2023. National Working Conditions Survey.
Yamada S, et al. (2023). The impact of age- and sex-specific reference ranges for serum TSH and FT4 on the diagnosis of subclinical thyroid dysfunction. Thyroid, 33(4).